We need to stop asking “GLP-1s or surgery?” for obesity.
That’s the wrong question.
The right question is: what does this patient need, at this stage of their disease?
Obesity is chronic, progressive, and heterogeneous. The era of picking a lane — medical or surgical — is over. The best outcomes come from building integrated pathways. Here’s how I think we could think about it clinically.
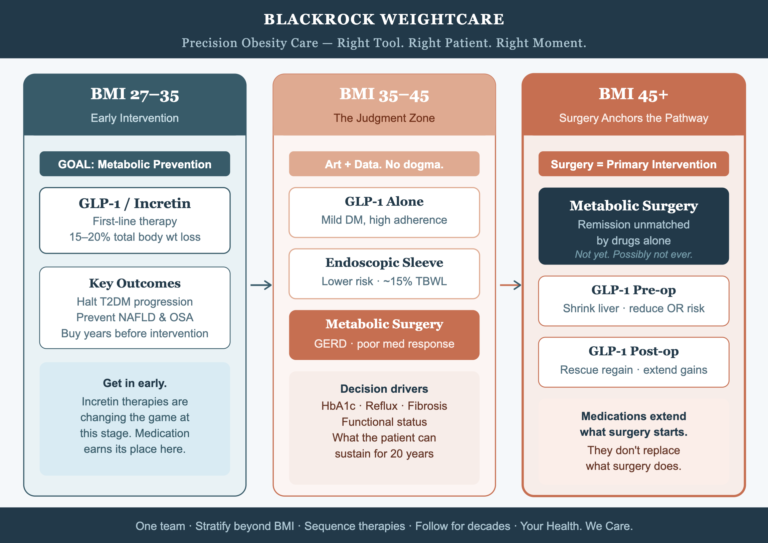
BMI 27–35: Early intervention, metabolic protection
This is where the newer incretin therapies have genuinely expanded our toolkit. For patients without advanced complications, GLP-1s can achieve meaningful weight loss and delay progression to T2DM, NAFLD, and OSA. The goal here is prevention — getting in early before the disease accumulates damage. Medication earns its place at this stage, and I use it.
BMI 35–45: The judgment zone
No dogma here. This is where clinical decision making meets outcome data.
I’ll consider GLP-1s alone when diabetes is mild or very recently diagnosed and the patient is highly adherent. Endoscopic options when they want a lower-risk bridge with 15% total body weight loss (TBWL). Surgery when there’s severe GERD, significant visceral fat, liver fibrosis, established diabetes or a poor response to medical therapy.
Often the sequence is: surgery for the durability that drugs alone haven’t matched long-term. HbA1c, reflux burden, functional status, and what the patient can realistically sustain for 20 years, cumulative cost of injectables — these also can drive the decision for surgery versus a trial of medication, not the BMI alone.
BMI 45+: Surgery anchors the pathway
The data here hasn’t changed, and it won’t be overturned by a few years of GLP-1 trial data. For severe obesity with end-organ damage — fatty liver disease, refractory T2DM, sleep apnoea, joint destruction — metabolic surgery delivers weight loss and disease remission at a magnitude we cannot replicate pharmacologically with medications available to date. Not yet. Possibly not ever, for this cohort.
That said, GLP-1s have earned a genuine role around surgery: shrinking the liver pre-operatively in very high BMI patients, reducing anaesthetic risk, and rescuing for weight regain long after the operation. They can extend what surgery starts. They don’t replace what surgery does.
What the best programs are building
Stratify by more than BMI — we need to stratify patients by metabolic burden, genetics, psychological readiness, and social context all matter. Sequence therapies deliberately and consider what the correct combinations are based on the stage of the disease. Follow patients for decades, not months. And put surgeons, physicians, dietitians, and psychologists in the same room, sharing the same data.
The tribalism between “medical” and “surgical” camps has cost patients. The win here is designing systems that deliver the right option, to the right patient, at the right moment in their disease trajectory.
That’s precision obesity care. And it needs surgeons to build it.
Your Health. We Care.